

The Adaptogen Problem

The term “adaptogen” is the most overused and least useful term in modern herbalism. You see it everywhere - marketing materials, product labels, blog posts, even in clinical conversations where it actively interferes with good decision-making. The adaptogen concept has confused practice and misdirected people for too long; it is time to put it to bed once and for all.
Clinical clarity matters. Vague, poorly-defined terms that promise everything and differentiate nothing lead to worse decisions for the people we’re trying to help. Over the next 15 pages, I’ll show how the adaptogen concept fails clinically, phenomenologically, definitionally, historically, and evidentially.
The Clinical Problem: A Term That Fails to Differentiate
Almost every other term we use in Western herbalism serves a clear clinical function. These terms help us differentiate what plants do so we can make informed choices.
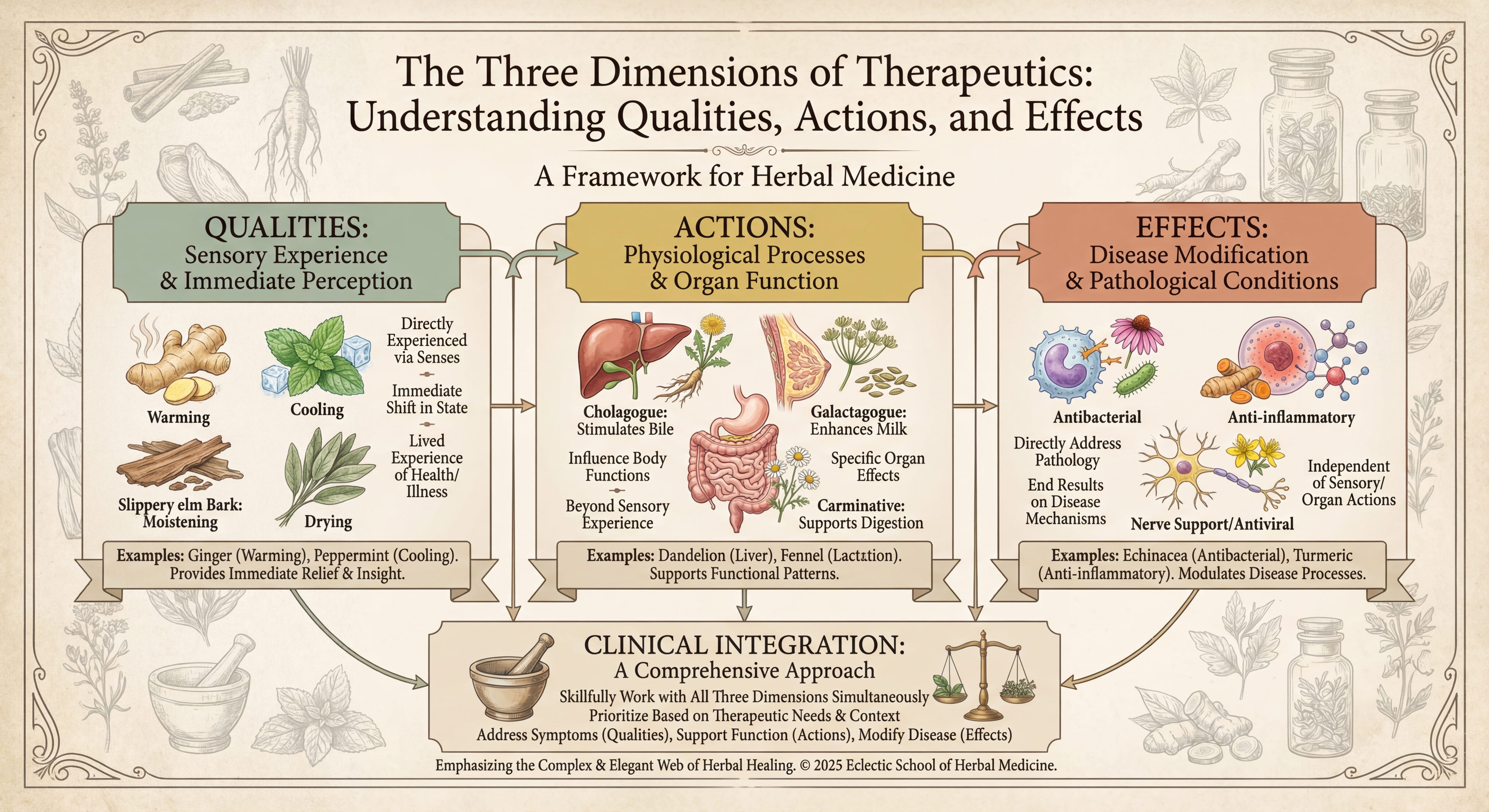
Take qualities. When I say a plant is cooling, you know I’m not talking about something warming. Moistening means not drying. These perceptible states have immediate therapeutic relevance. You can feel the cooling of peppermint, the warming of ginger, the drying of sage, the moistening of marshmallow. That embodied feedback matters clinically because you can tell whether you’re moving someone’s experience in a helpful direction.
Then we have action terms - cholagogue, galactagogue, diuretic, expectorant, antispasmodic. These describe what herbs do to specific tissues or physiological functions. You can often feel these actions (the relaxation from an antispasmodic, the increased urination from a diuretic) and sometimes measure them directly (bile flow, milk production, urine output). Each term narrows down our choices and helps us match herbs to actual clinical needs.
Finally, effect terms describe impacts on disease processes - antibacterial, anti-inflammatory, antifungal. These identify specific, measurable outcomes on pathology. An antibacterial herb might not be anti-inflammatory. An anti-inflammatory herb might not be antibacterial. The terms tell us something specific.
This three-dimensional system - Qualities, Actions, and Effects - lets us identify herbs that will reliably shift experiential states, support specific organ systems, and in some instances, address disease processes directly. Each term narrows our choices and helps match herbs to real clinical situations.
But then we get to “adaptogen” - a term that doesn’t fit anywhere in this framework.
You can’t perceive it as a quality. It doesn’t specify which tissues or functions are affected. It doesn’t identify a particular disease process being addressed. Instead, some vague, broad ability to “help the body adapt to stress” or “normalize physiological functions” without explaining mechanism or differentiating between plants.
So what does “adaptogen” actually mean clinically? Who gets it? More importantly, who doesn’t? If someone comes to me exhausted and burned out, should I give them an adaptogen? What if they’re anxious and wired? What if they’re depleted and cold versus inflamed and hot? What if they have insomnia versus hypersomnia? The term offers no guidance.
This matters more than semantics. When a practitioner says “I gave them an adaptogen,” I have no idea what they actually did or why. Did they give Ashwagandha? Rhodiola? Schisandra? Eleutherococcus? These plants have dramatically different qualities, actions, and effects. The term “adaptogen” lumps them together based on a 1950s Soviet theoretical framework that obscures their actual differences rather than clarifying specific uses.
The Phenomenological Problem: These Herbs Feel Wildly Different
If adaptogens really represented some meaningful category of plants with similar effects on the stress response, you’d expect them to feel similar when you take them. They don’t. Not even remotely.
Ashwagandha tends to be calming, sometimes sedating, often helpful for anxious, wired states. Many people find it helps with sleep. Rhodiola, by contrast, is often stimulating, can increase energy and alertness, and may worsen anxiety or insomnia. Schisandra has a notable sour taste and appears to have biphasic effects - relaxing and calming at lower doses, but distinctly stimulating at higher doses, which fits with its original classification as a stimulant in Soviet research. Eleutherococcus is generally considered mildly stimulating.
We’re calling plants with opposite phenomenological effects by the same name. One makes you sleepy, another keeps you awake. One calms you down, another amps you up. The lived experience of taking these herbs is completely different.
Someone who is anxious, agitated, and not sleeping needs something fundamentally different than someone who is depleted, exhausted, and struggling with low energy. Calling both situations “stress” and both sets of herbs “adaptogens” actively interferes with making good matches.
And then there’s the dose-dependent complexity. Schisandra at low doses might provide some calming support, but push the dose higher and you’re looking at stimulation, potential insomnia, agitation - that doesn’t fit with the idea of an herb that intelligently “adapts” to what someone needs.
The phenomenological diversity among so-called adaptogens suggests we’re not dealing with a meaningful category. We’re dealing with plants with diverse qualities and actions that have been artificially grouped together based on theory rather than observable effects.
The Definitional Incoherence: Non-Specific Effects That Are Somehow Also Specific
Let’s look at how adaptogens are typically defined. The classic definition, from Brekhman and Dardymov’s 1969 paper, states that adaptogens must:
Be non-specific and help the body resist a wide variety of stressors
Have a normalizing influence independent of the nature of the pathological state
Be innocuous and cause minimal disorders in physiological functions
There’s a fundamental logical problem here. How can something have “non-specific” effects on stress while also having specific effects on particular conditions? Yet this is exactly what adaptogen research claims.
Look at the modern research on these plants. Ashwagandha is studied for anxiety. Rhodiola for depression and fatigue. Schisandra for cognitive function. These are specific effects on specific conditions. The research doesn’t show these plants “normalizing” everything - they have particular effects on particular problems, breaking the definition.
And then there’s the “innocuous” part. These plants aren’t always innocuous. We have documented case reports of serious harm. Ashwagandha has been associated with thyrotoxicosis in multiple published cases - thyroid storm severe enough to require hospitalization. There are case reports of acute psychosis following ashwagandha withdrawal. Rhodiola has triggered manic episodes in people with bipolar disorder. Chronic high-dose use of Panax ginseng produces Ginseng abuse syndrome - with symptoms including insomnia, hypertension, edema, skin eruptions, and morning diarrhea.
These aren’t side-effect-free substances that gently nudge everything toward balance. They have real, specific effects - and real potential for making some people significantly worse if used inappropriately. Calling them “innocuous” when we have case reports of thyroid storm, psychosis, and mania is both inaccurate and dangerous.
The adaptogen definition promises a kind of herbal panacea that doesn’t exist - plants that somehow transcend the normal rules of pharmacology and can intelligently sense what each individual person needs. This is magical thinking. I have no problem with magical thinking. Some people need more magical thinking and enchantment. But be honest about it. Find a nice amulet. Better yet, a nice house plant. Don’t pay supplement prices for enchantment while pretending you’re doing traditional herbal medicine.
The Practical Incoherence: Who Actually Needs These?
Let’s push on the adaptogen concept and force it to commit to something testable. Because right now it enjoys the luxury of vagueness - broad enough to never be proven wrong, which is a hallmark of pseudoscientific thinking.
The core claim is that adaptogens help the body cope with stress. Fair enough. But let’s follow that thought for a moment. Who experiences chronic stress in modern life? Essentially everyone. Work stress, financial stress, relationship stress, health stress, news-cycle stress, climate anxiety - pick your poison. If adaptogens address “the effects of stress,” and stress is nearly universal, then the logical conclusion is that adaptogens are necessary for nearly everyone.
Is that the claim? Should everyone be taking adaptogens?
The most prolific researcher/writer on adaptogens, Panossian says
The prophylactic use of adaptogens seems to be justified in healthy subjects for preventing aging-related diseases, and to attenuate stress-induced harmful effects.
So yes - the claim is everyone should be taking adaptogens, even healthy folks. So which adaptogens? Ginseng, starting with the introduction of solid food, or before? Ashwagandha for the anxious ones and Rhodiola for the depleted ones? What about people who are both anxious and depleted at different times of day? All of them in rotation? In what doses? For how long - forever, since stress isn’t going away? What happens when you stop? The concept offers no guidance because it was never designed to answer practical questions. It was designed to sell products.
And if everyone should be taking adaptogens, what weight of evidence would we expect to support such an extraordinary claim? When we say something benefits nearly everyone, that’s a massive assertion requiring proportionally robust evidence - large trials, replicated findings across different populations, clear dose-response relationships, long-term safety data. Instead, we have a number of trials that found no benefit, or found harm, no one wants to talk about, along with mountains of methodologically flawed Soviet research, a handful of positive industry-funded studies with conflicts of interest and, and multiple expert panel reviews of all available information explicitly stating the evidence doesn’t support efficacy claims. That’s the evidence base for a universal recommendation?
But maybe the claim isn’t that everyone needs adaptogens. Let’s set aside the opinion of the guy who’s built his whole reputation and career on the supposed efficacy of adaptogens and say the claim is more modest - just that they’re beneficial for people under significant stress. Okay, let’s work with that. Which people specifically? How do we identify them?
Is there a stress scale where, once you hit a certain threshold, adaptogens become warranted? Where is this threshold? What validated instrument measures it? The Perceived Stress Scale? The Holmes-Rahe Life Stress Inventory? Salivary cortisol levels? Some combination? I’ve never seen an adaptogen proponent specify what level of stress justifies adaptogen use, because that would require the kind of precision the concept can’t provide. It would also open up the uncomfortable question of what evidence demonstrates adaptogens help people above this threshold but not below it. That evidence doesn’t exist because the question has never been seriously asked.
Let’s say we accept, for the sake of argument, that adaptogens provide some benefit for stressed people. We still need to ask: compared to what? Among all the interventions considered beneficial for people under chronic stress - and there’s actually decent evidence for many of them - where do adaptogens rank?
Consider the things we know help with chronic stress: adequate sleep, regular movement, social connection, time in nature, reduced workload, nutrient-dense food, stress-reduction practices, meaningful work, financial stability. These aren’t exotic interventions. They’re foundational. And for all of them, we have substantially better evidence than we have for adaptogens.
But let’s stay in supplement territory for a moment, since that’s where adaptogens live. People often reach for adaptogens when they’re fatigued, mentally foggy, or feeling depleted. Fair enough - those are real problems worth addressing. But where would you rank adaptogens among your interventions for fatigue?
Take creatine. There’s reasonably strong evidence that creatine supplementation reduces cognitive fatigue, particularly under conditions of sleep deprivation or mental exhaustion. Multiple well-designed studies show improvements in working memory and processing speed when people are stressed or sleep-deprived. The mechanism is plausible - creatine supports ATP regeneration in the brain, and cognitive work is metabolically expensive. The effect sizes are modest but consistently replicated across independent research groups.
Or consider theanine. The evidence base shows improvements in stress levels and sleep quality. The mechanism makes sense - theanine promotes alpha wave activity and supports GABA function without sedation. Multiple independent trials, reasonable sample sizes, plausible pharmacology.
I’m not saying creatine and theanine are miracle supplements. They have modest effects for specific applications. But that’s exactly the point - we can describe what they do, for whom, through what mechanism, with what quality of evidence. Try doing that with “adaptogens.” The specificity disappears into vague claims about “supporting the stress response” and “normalizing function.”
If someone comes to me exhausted and depleted, and I’m thinking about supplements (after addressing sleep, nutrition, and the other foundational factors), I can make a reasoned case for creatine based on its evidence for cognitive fatigue. I can consider theanine if sleep quality seems like the rate-limiting factor. What’s the reasoned case for “an adaptogen”? Which one? Why that one over another? The framework gives me nothing to work with.
I’m a clinician working with real people who have to make real decisions. A few practical questions about adaptogens I’ve never seen addressed:
Should someone work longer hours to make more money to afford adaptogens? Supplements are expensive, and many people are choosing between financial priorities. If someone works an extra two hours a week to pay for their adaptogen habit, are they better off than if they’d used those couple of hours for sleep, movement, or time with people they care about? I’d bet heavily on the latter, but the adaptogen framework can’t even engage with this question because it treats these herbs as a special category rather than one option among many.
What if someone can afford fresh vegetables or adaptogens, but not both? Which gets priority? I think the answer is obvious, but I’ve watched people make the opposite choice because marketing has convinced them adaptogens are essential while vegetables are just, you know, food. The adaptogen concept, by positioning these herbs as uniquely important for stress, distorts reasonable priority-setting.
What’s the evidence that adaptogens provide more benefit per dollar than an extra hour of sleep per night? Than a daily walk? Than weekly time with friends? These comparisons are never made because adaptogens exist in a marketing bubble where they’re not competing against the mundane interventions that actually form the foundation of stress resilience. The concept insulates itself from practical cost-benefit analysis.
Any answer to these questions exposes the problem. If the answer is “everyone should take adaptogens,” that’s an extraordinary claim the evidence doesn’t support. If the answer is “only some people,” then we need specificity the concept refuses to provide. If the answer is “it depends on the individual,” then congratulations - you’ve just described every herb, and the term “adaptogen” isn’t doing any clinical work. It’s not differentiating. It’s not guiding decisions. It’s just... there, sounding vaguely scientific while meaning nothing precise.
A concept that can’t be pinned down to testable claims, that can’t specify who benefits and who doesn’t, that can’t be compared against alternatives, that can’t guide practical priority-setting… If you look closely at the concept of adaptogens, what you really find is clever marketing copy dressed up in scientific language, not a clinical concept.
The Historical Problem: Stimulants Rebranded
Many of these plants, later called adaptogens, were already being studied for other effects and got relabeled when a new theoretical framework emerged.
Research on Schisandra was formally initiated during World War II by Order 4654-p, which mandated studies “to study the Chinese herb Limonnik with the purpose of determining its possible use as a raw material for obtaining organic acids, ether oils and tonic substances.” During the initial research period from 1943-1947, Soviet scientists described Schisandra’s “stimulating activity” or “stimulatory effects” - not adaptogenic properties.
Why? Because the term “adaptogen” didn’t exist yet. It wasn’t published in scientific literature until 1958. Before that, Schisandra was studied and classified as a stimulant. It was recognized for causing, in larger doses, insomnia and agitation - effects we associate with stimulants, not with herbs that “normalize” stress responses.
So what changed? The adaptogen concept emerged in the late 1950s, was formally defined in 1969, and these existing stimulant herbs were retrospectively reclassified. Schisandra didn’t change. Its effects didn’t change. But the language used to describe it shifted from “stimulant” to “adaptogen.”
This matters more than you might think. When you call something a stimulant, practitioners know to be cautious about using it in people who are already wired, anxious, or not sleeping. When you call it an adaptogen, that caution disappears. The term suggests it will somehow intelligently adapt to what the person needs, when in reality you’re still looking at stimulating effects for many people - especially at higher doses where Schisandra’s biphasic nature shows its stimulant face.
The adaptogen concept emerged from Soviet research looking for ways to enhance soldier and worker productivity - substances that could help people work harder, longer, in difficult conditions. The goal was pushing through, not healing or building resilience.
The same Soviet labs that turned Schisandra into an “adaptogen” were also testing synthetic drugs like dibazol, bemitil, and bromantane AS ADAPTOGENS. If you wouldn’t be comfortable taking Soviet era performance enhancing drugs based on the strength of that research alone, it’s worth asking why the label feels so convincing when it’s attached to herbs.
The Research Quality Problem: Methodological Disasters and Acknowledged Flaws
The research base that supposedly supports the adaptogen concept is deeply flawed, and even the field’s leading researchers acknowledge this.
Alexander Panossian is arguably the most prolific adaptogen researcher, with approximately 200 publications on the topic. He’s been instrumental in promoting the adaptogen concept and has served as Head of Research & Development for the Swedish Herbal Institute (more on them shortly). If anyone has a vested interest in defending adaptogen research quality, you’d think it would be Panossian. Yet even Panossian admits that most of the Soviet-era trials were “poorly designed and conducted,” and summarized the USSR clinical studies as “the most questionable and poorly documented” in the entire adaptogen literature.
The problems extend well beyond the old Soviet data. In 2009, Blomkvist, Taube, and Larhammar published what is basically a forensic takedown of Rhodiola trials in Planta Medica. They went through seven “positive” studies and found serious problems in six of them. Not nitpicky details—things you’d expect in a sloppy student project, not in clinical research. Wrong or irrelevant statistics, trials with no placebo group, numbers and graphs that don’t match, conclusions resting on unpublished follow-up data, and a depression study where the placebo group somehow showed no improvement at all (which simply doesn’t happen in antidepressant trials).
Their bottom line was that these Rhodiola trials “are of poor scientific quality and their conclusions are not supported by the data.” And in four of the six problematic studies, a company that makes Rhodiola extract – the Swedish Herbal Institute – was involved, which only makes the whole situation look worse.
Short of outright accusing anyone of fraud, this is about as close as a formal paper gets to saying, “these results should not be trusted.” In any other field, a published criticism this harsh would be career-ending.
Multiple other systematic reviews have identified similar problems. Walker and Robergs (2006) found “equivocal results” and noted something curious - Eastern European studies consistently showed positive effects while Western European and North American studies “produced mixed results.” This geographic disparity in findings is a red flag. When research from one region consistently shows effects that other regions can’t replicate, you have to question the methodological rigor of that research tradition.
Hung, Perry, and Ernst (2011) found that only 5 of 10 randomized controlled trials scored above 3 on the Jadad scale (indicating good quality). Their major conclusion identified a critical problem: “The trials differed greatly in terms of condition tested, and independent replications of any given trial are missing.” They emphasized “a lack of independent replications of the single different studies.”
Ishaque et al. (2012) found that only 2 of 6 trials on physical fatigue showed Rhodiola effective, and only 3 of 5 trials on mental fatigue showed effectiveness. They concluded: “Research regarding R. rosea efficacy is contradictory,” and “While some evidence suggests that the herb may be helpful, methodological flaws limit accurate assessment of efficacy.”
The recurring methodological problems across these reviews include: small sample sizes, poor randomization, lack of blinding, short treatment periods, inappropriate statistical methods, selective outcome reporting, variable plant preparations, inconsistent extraction methods, different dosing regimens, and no independent replications.
What Good Trials Actually Show
It’s not just that the “positive” adaptogen literature is riddled with weak methods. What almost never gets talked about are the well-done trials where adaptogens either failed outright or actually made things worse.
1. Eleutherococcus for chronic fatigue – looked good… until you add placebo
Hartz et al. (2004, Psychological Medicine) randomized 96 people with idiopathic chronic fatigue or CFS to Eleutherococcus or placebo for two months. Both groups improved, but there was no difference at all between them on the primary fatigue scale in the full sample. The authors’ own conclusion: overall efficacy was not demonstrated; only a post-hoc subgroup with milder fatigue showed any signal.
2. Eleutherococcus added to stress management – the herb does nothing
Schäffler et al. (2013, Pharmacopsychiatry) put stressed employees into three arms: stress-management training alone, Eleutherococcus alone, or both together. Over 12 weeks, almost all parameters improved, but there were no meaningful differences between groups, and adding Eleutherococcus to a decent stress-management program gave no extra benefit. The authors summed it up: any effect of Eleutherococcus was “negligible.”
3. Rhodiola in nursing students – fatigue worse than placebo
Punja et al. (2014, PLOS ONE) randomized 48 nursing students on shift work to 42 days of Rhodiola or placebo. On both the SF-36 Vitality scale and a VAS for fatigue, placebo did better. By day 42, the change in fatigue scores was significantly in favour of placebo, leading the authors to state that Rhodiola worsened fatigue compared with placebo in this population (with all the cautious caveats you’d expect).
4. Ashwagandha for stressed, overweight adults – primary endpoint fails
Smith et al. (2023, Journal of Psychopharmacology) ran a 12-week double-blind RCT in 121 overweight or mildly obese adults aged 40–75 with high stress and fatigue, using a branded ashwagandha root extract (Witholytin®, 200 mg BID). Stress scores (PSS) fell in the ashwagandha group – but they fell just as much in the placebo group. The improvements on the primary outcome were not significantly different between groups (p = 0.867), even though this is exactly the kind of trial design adaptogen claims are supposed to shine in.
These are reasonably designed, placebo-controlled trials that go straight after the core promises of adaptogens – better fatigue, stress resilience, and energy – and either find no advantage over placebo or, in the case of Rhodiola in nursing students, a signal that people actually did worse on the herb.
The Conflict of Interest Problem: Commercial Entanglement
If you’re shaking your head and wondering how we got here, here’s where we name the problem - the extensive commercial conflicts of interest that permeate the field.
The Swedish Herbal Institute founded in 1975, describes itself as the “world leader in adaptogens” with “more than 35 years of research.” But this isn’t an independent research institution. It’s a commercial manufacturer with a GMP-certified manufacturing plant producing proprietary products sold internationally.
SHI’s flagship products are ADAPT-232 (sold as Chisan®), a combination formula of Rhodiola, Schisandra, and Eleutherococcus, and SHR-5 Extract, a proprietary Rhodiola rosea extract sold as “Arctic Root.” These products are marketed as “the only Rhodiola extract with proven efficacy in clinical studies published in international scientific journals.”
Alexander Panossian, the most prolific adaptogen researcher, served as Head of Research & Development for Swedish Herbal Institute from 2003-2016. During this period, he authored numerous papers testing SHI products while employed by the company manufacturing those products. In 2016, he founded his own R&D company, Phytomed AB, and became Head of Research & Development for EuroPharma USA Inc., another supplement manufacturer, while maintaining a consulting agreement with them.
Georg Wikman, co-author with Panossian on numerous papers, is the founder of Swedish Herbal Institute and developer of the ADAPT-232 formula. His institutional affiliation in publications is listed as “Swedish Herbal Institute Research & Development,” which obscures for many readers that this is a commercial entity rather than an independent research institution.
The same entity manufactures proprietary products, employs researchers, funds poorly designed research on its own products, publishes that weak research in peer-reviewed journals, then uses that research to market products with claims like “clinically tested” and “scientifically proven.” This creates a self-reinforcing system where studies authored by SHI-affiliated researchers cite other SHI-affiliated research.
Remember those four problematic Rhodiola studies identified by Blomkvist et al.? The Swedish Herbal Institute was involved in all four of them. Blomkvist shows a pattern where the same commercial entity repeatedly produces methodologically flawed research on its own products, publishes it, and uses it for marketing.
What This Means for Practice
So where does this leave us clinically? I think we need to make a clear distinction between the adaptogen concept and the actual plants that have been labeled with this term.
The adaptogen concept - this idea that certain plants have some special, non-specific ability to normalize stress responses and build resilience - lacks good supporting evidence. The term itself is clinically unhelpful because it doesn’t differentiate between plants with very different qualities, actions, and effects.
But that doesn’t mean these plants aren’t useful. We need to understand them based on their specifics rather than lumping them into a vague category.
Ashwagandha has documented effects on anxiety and sleep due to its calming, somewhat sedating properties. It also appears to have thyroid-stimulating effects, which means we need to be thoughtful about using it in people with hyperthyroidism or who are taking thyroid medication. And we have those case reports of thyrotoxicosis - not exactly an innocuous normalizer.
Rhodiola appears to have stimulating effects that might help some people with fatigue. This makes it potentially useful for someone who’s depleted and dragging, and potentially problematic for someone who’s already wired. We need to match the plant’s actual effects to what the person needs, not rely on ideas about intelligent adaptation. And we need to remember those case reports of mania in people with bipolar disorder.
Each plant, evaluated on its own, outside of a clinically useless concept.
When I work with someone experiencing what we might broadly call “stress,” I don’t reach for an adaptogen. I try to understand their specific experience. Are they wired or tired? Hot or cold? Tense, agitated, ruminating, catastrophising? Sleeping poorly because they can’t fall asleep, or because they can’t stay asleep? Are they anxious, depressed, or both? What’s their energy pattern throughout the day? What makes it better, what makes it worse? Even simple things like stress require thoughtful exploration.
After exploring I think about which herbs have qualities, actions, and effects that match what this specific person needs. The adaptogen framework suggests you could use the same herb for someone anxious and hot versus someone depleted and cold. That makes no clinical sense.
I also think we need to be honest about what herb can and can’t do. If someone is experiencing significant stress-related symptoms, the foundational interventions need to come first: sleep, nutrition, movement, stress regulation, connection, circadian rhythm support. These aren’t sexy interventions, but they’re more important than any herb. Herbs can support these foundational changes. They can’t substitute for them.
When someone’s stress symptoms are severe enough that basic lifestyle changes and herbal support for those lifestyle changes (gnaw on that a bit) aren’t sufficient, that person may need more than herbs. They may need therapy, medication, changes to work or living situations, or treatment for underlying conditions like thyroid dysfunction or anemia. Calling something an adaptogen and suggesting it will magically fix all causes of stress obscures when we’re out of our depth and referral is appropriate.
The Bigger Picture
The adaptogen problem is really a case study in how marketing can hijack language and muddy clinical thinking. The term sounds scientific. It references research. Companies can charge premium prices for “adaptogenic” formulas.
But look closely at what we’ve covered: incoherent definitional criteria, foundational research acknowledged by field leaders as methodologically flawed, high-quality studies showing null effects, and research heavily funded by product manufacturers.
We can do better. We can understand these plants based on what they actually do. We can make informed choices about when each might be helpful and when it might not. We can acknowledge uncertainty while making clinically sound decisions based on empirical observation.
Time to retire “adaptogen” to the category of historically interesting but clinically unhelpful concepts. Let’s talk about these plants in terms of what they actually do, for whom they might be helpful, and when we should use something else instead.
I'm so curious about this. I was taught by my first herbal studies teacher (trained clinically but teaching out of folk/community herbalism lineage) that adaptogens are herbs that help bring the body back to homeostasis by nourishing and supporting the adrenals. Sort of analagous, I thought, to how a hepatic does the same for the liver. And so for depleted, stressed out, overtaxed etc. nervous systems you want to nourish your adrenals (among other things). The plants you mention here were not in our materia medica, the teacher was talking about nettles, whole plant dandelion, borage, licorice root, staples in my materia fornlots of reasons.
As I have learned more, from other teachers, I've been questioning some of the things taught by that first teacher, as being, hmm, insufficient for understanding A&P and herbal actions, and sometimes coming out of these kind of unfounded claims that sound nice but aren't grounded in much more than...vibes. It's annoying to unlearn/relearn but makes me a better herbalist.
At any rate, I guess my question is, is there anything useful about how I was taught to understand adaptogens? Or are there more specific ways to understand what these plants are doing in the body that, oh yeah, also help the stressed out adrenals recover?
Thanks for this piece!
People think any “adaptogen” is good medicine for everybody. It's insane.